Why Does It Hurt When I Breastfeed and How Can I Improve the Latch?
By: Shoshy Neubauer - IBCLC Certified Lactation Consultant
Breastfeeding pain is one of the most common complaints among mothers, especially in the first days and weeks postpartum. Although the phrase "breastfeeding shouldn't hurt" is commonly heard, the reality is that many mothers experience pain, frustration, and injuries. It is important to distinguish between the natural tenderness of the first few days and sharp or continuous pain. While mild tenderness at the beginning of suckling (which passes within a few seconds) is a normal phenomenon resulting from tissue adaptation, burning, pinching, or pain that lasts throughout the entire nursing session is a clear sign that something in the breastfeeding mechanism requires readjustment. Understanding the source of the pain and applying techniques to improve the latch are the key to nourishing, effective, and pain-free breastfeeding.
The Source of Pain: Why Does It Happen?
To resolve the pain, we must first understand the mechanics of the baby's mouth and the breast. Here are the primary causes of breastfeeding pain:
1. Shallow Latch - The #1 Cause of Pain:
This occurs when the baby grasps only the tip of the nipple instead of a large area of breast tissue and the areola. In a normal state, the nipple should reach deep into the baby's oral cavity, to the area of the soft palate (the back part of the roof of the mouth). When the latch is shallow, the nipple remains in the hard palate area, being abraded and crushed between the tongue and gums with every suckling motion


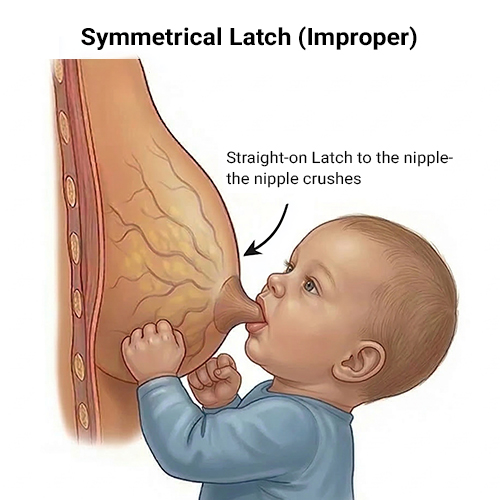
2. "Symmetrical" Latch to the Breast:
When you bring your baby to the breast, if the mouth attaches directly to the nipple, the baby's lower palate and tongue will press against the nipple -which is densely populated with nerve endings - causing pain and potential injury. However, when you position the baby at the correct height with the nose aligned opposite the nipple, the lower jaw and tongue remain clear of the nipple and will not cause trauma. Consequently, you will not experience pain.

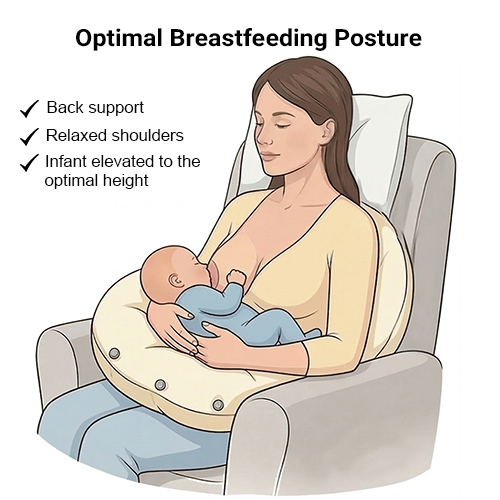
3. Inaccurate Positioning and Posture
Breastfeeding requires precise spatial alignment between the mother and the baby. Many mothers tend to lean forward toward the baby, which distorts the angle of the breast's entry into the baby's mouth, creates tension in the mother's muscles, and leads to a shallow latch that causes friction and pain. A suitable breastfeeding pillow can assist in maintaining a comfortable seated position and aligning the baby correctly with the breast.

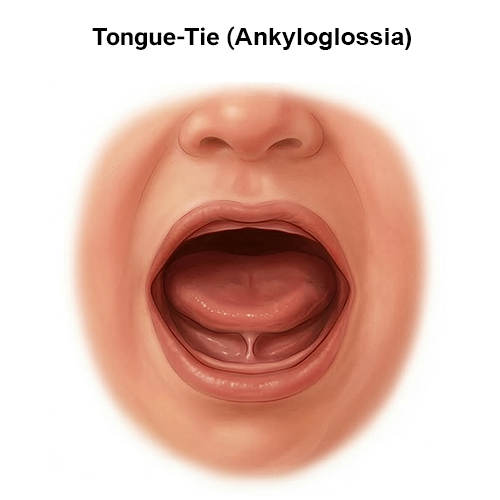
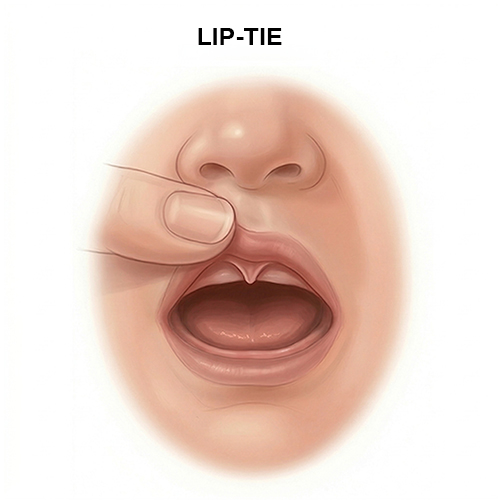
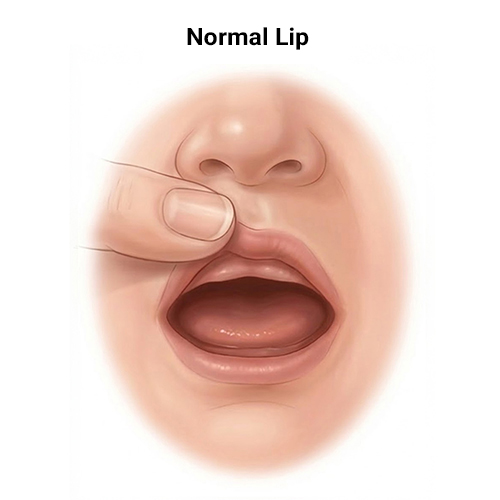
4. The Baby's Anatomical Challenges:
Conditions such as a tongue-tie (Ankyloglossia), lip-tie, or an unusually high palate can limit the baby's ability to create an effective vacuum and wrap around the breast properly, causing them to compensate by "biting" the nipple with their gums.
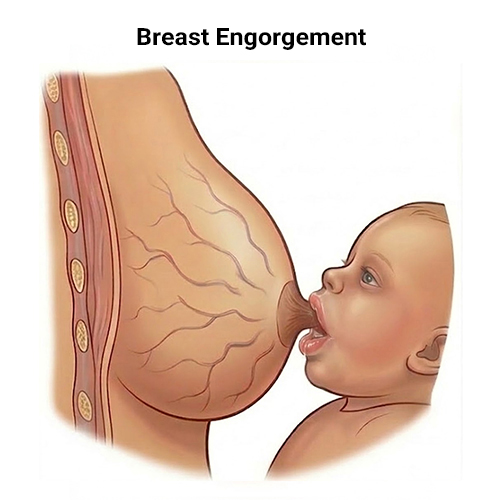
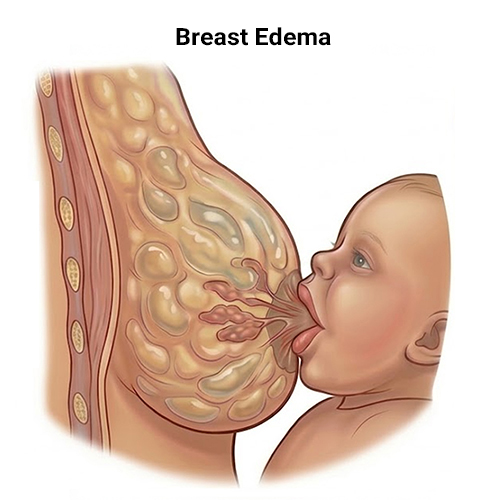
5. Engorgement, Fullness, or Edema:
During the days when the milk "comes in" (typically days 3–5 postpartum) or following a prolonged interval between feedings, the breast may become very firm and engorged. In this state, it is difficult for the baby to achieve a deep latch, much like the difficulty of taking a bite out of a large, hard apple.
6. Maternal Medical Conditions:
Pain can also stem from a breast yeast infection/thrush (usually characterized by a stabbing or burning pain or itching even between feedings, and sometimes accompanied by a shiny or peeling areola), or vasospasm (blood vessel constriction in the nipple, manifesting as a sharp pain and a change in nipple color to white after breastfeeding).
Why does it hurt when I breastfeed?
Summary of the most common causes| Cause of Pain | Why Does It Hurt? | How Should It Be? |
|---|---|---|
| Shallow Latch | The baby grasps only the tip of the nipple, which remains in the hard palate area, being abraded and crushed between the tongue and gums with every suckling motion. | The nipple should reach deep into the oral cavity, to the soft palate area. The baby grasps a large area of breast tissue and the areola. |
| "Symmetrical" Latch to the Breast | The baby's mouth connects directly to the nipple, causing the lower jaw and tongue to strike it directly (in an area full of nerve endings), which can injure it. | The baby is at the correct height (nose opposite the nipple), so the lower jaw and tongue are far from the nipple and do not strike it. |
| Inaccurate Positioning and Posture | The mother leans forward toward the baby, distorting the breast's entry angle, creating muscle tension for the mother, and leading to a loose latch and friction. | Correct spatial coordination: The mother leans back, and the baby is brought to her and well-supported, without straining the mother's muscles. |
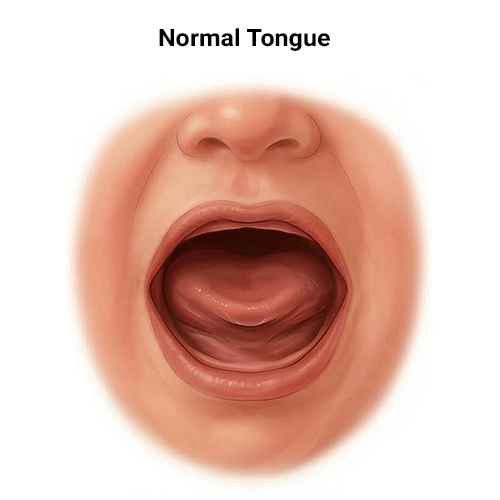
| Anatomical Challenges (Tongue/Lip Tie) | A movement restriction prevents the baby from creating an effective vacuum and wrapping the breast. The baby compensates by "biting" the nipple with their gums. | A flexible tongue allows for effective vacuum suckling and full breast wrapping (requires diagnosis and treatment if necessary). |
| Engorgement, Fullness, or Edema | The breast is very firm and tight, making it hard for the baby to grasp it deeply (much like biting into a hard apple). | A relatively soft breast, allowing the baby to grasp a deep portion of breast tissue (usually requires softening the breast prior to nursing). |
| Medical Conditions (Thrush, Vasospasm) | Thrush causes stabbing, burning, or itching pain. Vasospasm (blood vessel constriction) manifests as sharp pain and the nipple turning white after nursing. | Breast and nipples without unusual nerve sensitivity and free of infection (requires diagnosis and specific medical treatment for the mother). |
The Practical Guide - How to Improve the Latch Step by Step
Improving the latch starts even before the baby connects to the breast. A deep, asymmetrical latch is our goal. Here is how to do it correctly:
Step 1: Identifying Early Hunger Cues
Do not wait for the baby to cry. Crying is a late hunger cue. A crying baby is a frustrated baby who is difficult to soothe and comfortably latch onto the breast. Look for signs such as rooting motions, bringing hands to the mouth, and lip smacking.
Step 2: Positioning and Establishing Ergonomic Support
The foundation of successful breastfeeding lies in your posture. Sit comfortably, lean back, and bring the baby toward you - rather than the other way around. To maintain the proper height that allows the baby to reach the breast without you having to hunch forward, it is recommended to utilize dedicated support. The use of a firm, ergonomic breastfeeding pillow, such as Qualita’s MoonLove pillow (which allows for precise adjustment of the filling and features snap fasteners to secure its position), helps align the baby directly with the nipple. This relieves the strain on your shoulders and back, allowing you to control the breast's presentation angle in an optimal and relaxed manner.
Step 3: The "Ear, Shoulder, and Hip in One Line" Alignment
The baby's entire body should be facing you. Ensure that their ear, shoulder, and hip are in a straight line (Alignment). If their head is turned to the side while their body is lying flat on their back, it will be difficult for them to swallow, just as it is difficult for us to drink a glass of water with our heads turned to the side.
Step 4: "Nose to Nipple"
Position the baby so that their nose is located opposite your nipple. This starting position forces them to tilt their head slightly backward (Sniffing position). The backward tilt frees their chin and prompts them to open their mouth wider.
Step 5: Asymmetrical Latch
When the baby opens their mouth very wide (like a broad yawn), bring them to the breast with a firm yet gentle movement from the nape of their neck (and not from the head). Their chin should be the first to press deep into the lower breast, so that their lower lip takes in a large portion of the areola. The nipple will be directed upward, toward their upper palate.

Indicators of a Good and Effective Latch: How Will You Know You Succeeded?
✔️Sensation: You feel pulling and a vacuum, without pinching, rubbing, or sharp pain.
✔️Appearance of the Mouth: The baby's mouth is wide open (over 140 degrees), and their lips are flanged outward ("fish lips").
✔️Areola Coverage: More of the areola is visible above the baby's upper lip than below their lower lip (because the chin is buried deep in the breast).
✔️Sounds: Rhythmic and clear swallows can be heard. No clicking sounds (which indicate breaking the vacuum) are heard.
✔️Appearance of the Nipple at the End: The nipple comes out round and elongated. If it is crushed, white, or looks like a "slanted lipstick," the latch was too shallow.
✔️Appearance of the Mouth: The baby's mouth is wide open (over 140 degrees), and their lips are flanged outward ("fish lips").
✔️Areola Coverage: More of the areola is visible above the baby's upper lip than below their lower lip (because the chin is buried deep in the breast).
✔️Sounds: Rhythmic and clear swallows can be heard. No clicking sounds (which indicate breaking the vacuum) are heard.
✔️Appearance of the Nipple at the End: The nipple comes out round and elongated. If it is crushed, white, or looks like a "slanted lipstick," the latch was too shallow.
Questions & Answers (FAQ)
I latched the baby to the breast, but it hurts a lot from the very first moment. Should I wait for it to pass?
Absolutely not. If you experienced sharp pain immediately upon latching, do not suffer in silence hoping it will improve. Gently insert a clean finger into the corner of the baby's mouth to break the vacuum, detach them from the breast, and try to latch again. Practicing the correct latch prevents cumulative injuries.
How can you tell if the pain is due to an incorrect latch or a tongue-tie?
It is difficult to diagnose this alone. A tongue-tie restricts the mobility of the baby's tongue and will usually be accompanied by other signs: severe pain even though the latch looks good from the outside, a nipple that comes out crushed (lipstick-shaped), clicking sounds during nursing, or a baby who struggles to maintain a vacuum and detaches from the breast frequently. If you suspect this is the case, it is important to consult a certified lactation consultant (IBCLC) for a functional assessment of the tongue.
My nipples are already sore and cracked. What will help them heal?
The first and most important step to recovery is correcting the latch - because as long as the trauma continues with every feeding, the wounds will struggle to heal. Additionally, maintaining hygiene, applying a little breast milk to the nipple at the end of the feeding (air drying), or using coconut oil (which does not require washing off before the next feed) can provide significant relief. In the case of deep wounds or suspected infection, consult a professional.
Does the breastfeeding position really affect the pain?
Absolutely. The baby's body must be well supported so that they do not "hang" from the breast. When there is a gap between the mother's height and the baby's height, and the mother is forced to hold their weight in the air, the baby slides down, pulls the nipple, and injures it. Proper support of the baby's body completely changes the latch angle and prevents damage to the nipple. An ergonomic breastfeeding pillow (such as MoonLove) can facilitate appropriate support for both mother and baby.
The information presented in this article serves as a professional recommendation and does not constitute a substitute for individualized medical advice. In any case of unusual pain, bleeding, or persistent difficulty with breastfeeding, it is recommended to seek an evaluation from a certified IBCLC lactation consultant or your attending physician.
You are welcome to contact me:
Shoshy Neubauer, IBCLC Certified Lactation Consultant, Doula, and mother of 8.
054-5663700 [email protected] Facebook Instagram
Shoshy Neubauer, IBCLC Certified Lactation Consultant, Doula, and mother of 8.
054-5663700 [email protected] Facebook Instagram
More blog articles:
Symphysiolysis Dysfunction in Pregnancy: Everything You Need to Know - From Diagnosis to Perfect Sleep>
Breastfeeding Twins: Simultaneously or Separately – The Complete Guide for 2026>
The Complete Guide to Choosing a Pregnancy Pillow 2026: Which Pillow Shape Will Actually Help You Sleep?>Symphysiolysis Dysfunction in Pregnancy: Everything You Need to Know - From Diagnosis to Perfect Sleep>
